August 2023 Monthly Report



In this blog post, we discuss our August 2023 report and provide more information on how to interpret the results. The PDF report can be found at the end.
Key findings:
- The median fentanyl concentration found across all drug categories was 10.9%
- Carfentanil was not found in any samples
- Benzodiazepines and/or etizolam were found in 50% (165/333) of expected opioid-down samples
- Bromazolam, the most common benzo found within opioid-down, was found in 134 opioid-down samples with a median concentration of 3.9% and maximum concentration of 57.8%
- Xylazine was found in 29 samples (x27 expected opioid-down, x2 expected alprazolam) with a median concentration of 1.8% and a maximum concentration above 80% in an expected opioid-down sample
Insight for the August 2023 Monthly Report
This blog, and the associated pdf report, breakdown our sample counts into six categories:
-
samples received through direct service provision in Victoria, where service users are bringing samples into the Substance storefront. These samples are labelled as “Substance” samples in the figures/tables of this blog post
-
samples received through direct service provision in Campbell River, where service users bring samples to the Vancouver Island Mental Health Society (VIHMS). These samples are labelled as “Campbell River”.
-
samples received through direct service provision in the Comox Valley, where service users are bringing samples to AVI Health & Community Services in Courtenay, BC. These samples are labelled as “Comox Valley”.
-
samples received through direct service provision in the Cowichan Valley, where service users bring samples to the Duncan Lookout Society OPS in Duncan, BC. These samples are labelled as “Duncan”.
-
samples received through direct service provision in Port Alberni, where service users bring samples into Port Alberni Shelter Society’s OPS. These samples are labelled as “Port Alberni”.
-
samples received through indirect service provision, where samples are collected through no-contact drop-off envelopes, are collected by harm reduction workers and other community members at supported housing sites, overdose prevention sites, and supervised consumption locations. These samples are labelled as “Outreach” samples in the figures/tables herein. August’s Outreach data includes samples collected at the International Overdose Awareness Day BBQ, REVERB at Phillips Backyard, and Samsara Music Festival. Samples were also collected at Cumberland Wild Music Festival, these are labelled as “Comox Valley” samples
Drug types
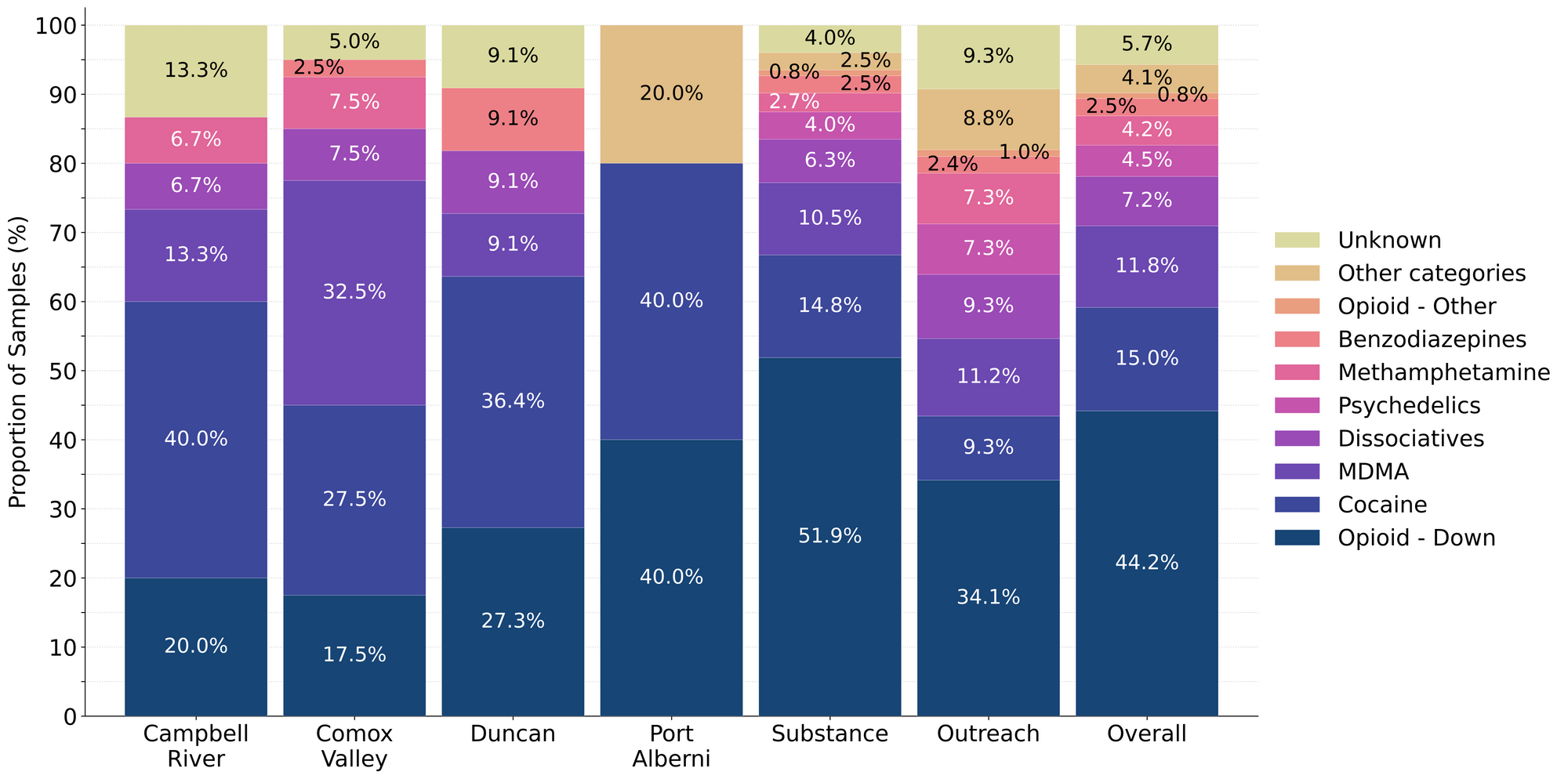
Fig. 1 shows the prevalence of each expected drug category checked, split by sample collection location/method.

August's Audacious Abstract of Actives a.k.a. The Sample Summary
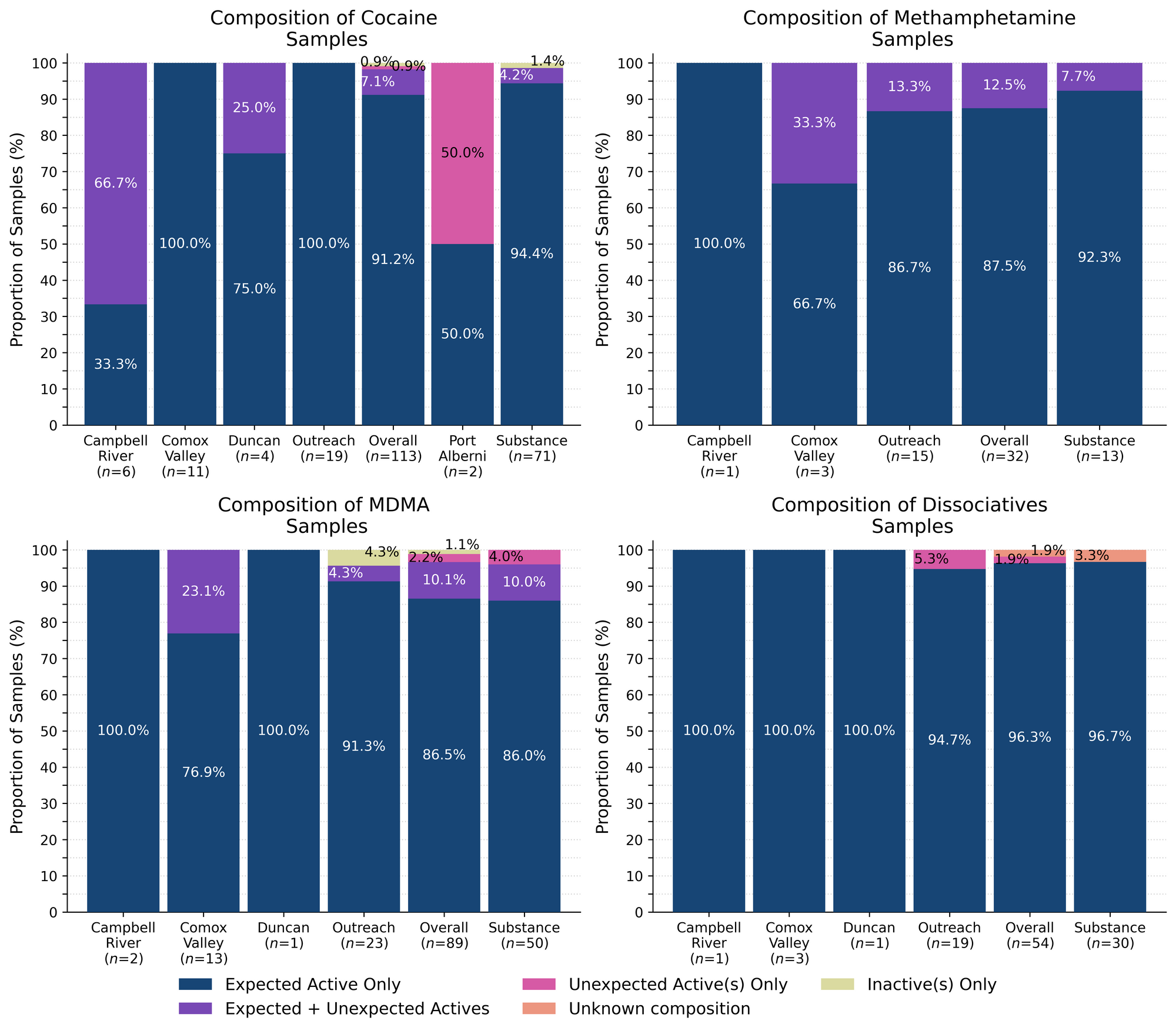
For the majority of samples checked, we confirm the presence of the expected drug with no additional active compounds detected above the limitations of the drug check. The bar charts below highlight a few classes of drugs, differentiating samples where only the expected active component was detected - from situations when other unexpected active components were detected.
98% (51/53) of expected ketamine samples checked in August were confirmed to be ketamine with no other active compounds detected.
Within the remaining two expected ketamine samples:
- One expected ketamine sample was found to contain MDMA and Dextrose (a sugar that is often made from corn or wheat). Some might consider that a sweet surprise and others might find that joke a little too corny.
- The last expected ketamine sample could not be checked due to too little of the substance to analyze beyond a fentanyl strip test (which was negative).
91% (103/113) of expected cocaine samples (90 cocaine HCl/soft, 23 cocaine base/hard/crack) were confirmed to be cocaine with no additional active compounds detected. One of these samples (from Victoria) contained an inactive cutting agent, inositol, at 23%. Inositol is a sugar that is found in some foods, such as dried prunes.
8 samples contained an active component in addition to cocaine:
- Benzocaine - One sample (Victoria); a topical local anesthetic. This sample contained around 80% benzocaine
- Phenacetin - Six samples (x1 Duncan, x2 Victoria, x3 Campbell River); “super buff” a Tylenol-like drug, commonly seen as a cut in cocaine. Phenacetin concentrations ranged from around 3% to 48%
- Benzodiazepine (Undifferentiated) - One sample (Campbell River); Further information regarding this sample is lacking.
One expected cocaine sample did not contain cocaine. This sample was a hard white pebble from Port Alberni that was found to be meth instead of cocaine. Finally, one expected cocaine sample was found to contain an unknown carbohydrate and an unknown oil, with no active drugs detected.
88% (28/32) of expected methamphetamine samples checked were found to be meth with no other active compounds detected. No inactive cuts were detected in these samples. In the four remaining samples, meth was found in addition to other active compounds:
- Two samples contained an undifferentiated benzodiazepine in addition to meth
- Of these two samples, one contained fentanyl or a fentanyl analogue
- An additional sample contained fentanyl or a fentanyl analogue in addition to meth
- One sample contained 2C-B in addition to meth
87% (77/89) of expected MDA/MDMA samples checked were confirmed to be MDA (4 samples) or MDMA (73 samples) as expected. The remaining expected MDA/MDMA samples displayed a range of compositions:
- Two expected MDA samples were found to contain additional active components. One of these samples contained ketamine while the other contained MDMA. Both samples were from the Comox Valley.
- One expected MDA sample submitted as a gummy was found to contain sucrose (sugar). We couldn’t detect any active components.
- Five expected MDMA samples were found to be mixtures of both MDA and MDMA. All were checked in Victoria.
- One expected MDMA sample from Campbell River was found to be a mixture of both cocaine HCl (8%) and MDMA (92%).
- One expected MDMA sample from Samsara Music Festival possibly contained an unknown cathinone, yet not one that was on our PS-MS target list.
- One expected MDMA sample was found to be cocaine HCl instead.
- One expected MDMA sample was found to be MDA instead.
Benzodiazepines (n=19)
79% (15/19) of the expected benzodiazepine samples checked in August came to our service sites in the form of pressed pills with the following expected and detected compositions:

Within the remaining four samples:
- One sample from Victoria was expected to be bretazenil. We could not detect any of the expected active, nor could we detect any other active components found on our PS-MS target list.
- One expected bromazolam sample was found to contain primarily bromazolam (>80%), fentanyl (approximately 2%), and caffeine. This sample was a light brown powder and was checked in Victoria.
- One sample was found to contain bromazolam. This sample also tested positive for fentanyl via a strip test, yet no evidence of fentanyl was found on PS-MS, this is likely due to cross-contamination between samples.
- One sample didn’t contain any benzos at all, it instead contained methamphetamine. This sample was a clear crystal and was checked in Victoria.
Opioid-positivity in non-opioid-down samples
In August, we checked 378 samples that were not expected to contain fentanyl or other “unexpected” opioids[1]. Since the opioid-down supply is no longer “just heroin” or “just fentanyl” and is instead a complex, potent, and ever-changing polysubstance market containing other synthetic opioids like fluorofentanyl or nitazenes, here we will examine the prevalence of any unexpected opioid, not just fentanyl, detected in non-opioid-down samples.
Specifically, we are excluding samples that were expected to be “opioid-down” or samples that had an “unknown/missing” expected composition. In the case of “opioid-other” samples, e.g. hydromorphone tablets and oxycodone pills, “unexpected opioids” are defined as any opioid that is not the expected opioid. ↩︎

Examining Table 3, we find that five samples tested positive for unexpected opioids in August, representing 1.3% of all non-opioid-down samples checked. These samples were as follows:
- Two were expected methamphetamine samples. Both tested positive for fentanyl via strip test however no fentanyl was detected via mass spectrometry
- Two were expected benzo samples
- One was an expected bromazolam sample which contained approximately 2% fentanyl. This sample was discussed in the previous section.
- One was an expected unspecified benzo sample that tested positive for fentanyl via a strip test, yet no evidence of fentanyl was found on PS-MS, this is likely due to cross-contamination between samples. This sample was also discussed in the Benzodiazepines section.
- One expected Oxycodone sample was found to contain metonitazene at 11% concentration instead. This sample was checked in Victoria and was a light blue-grey pill inscribed with “M” on one side and “30” on the other.
In August, no unexpected opioids were detected in samples expected to be cocaine, MDMA, dissociatives, or psychedelics.
In people’s personal quests for bodily autonomy and informed consumption, there is often evaluation of risk and consequence, but when the consequences can be severe and the risks are unknown or are intentionally exaggerated, these become difficult, if not impossible, conversations to weigh. We believe that drug checking can help provide people with the information needed to evaluate the risks, and provides harm reduction advice to minimize undesired consequences of substance use. These data are not meant to downplay concerns or invalidate past experiences. We recognize the tragic consequences of when fentanyl is found in non-opioid samples and honour the heartbreak that such experiences produce. Instead, we present these data with the intent to combat misinformation and provide an evidence-based context for people to consider when making decisions about substance use. While these numbers reflect what we have seen over the course of the project, these (roughly) 1-in-100 events still occur, so we always encourage folks to get their stuff checked.
Opioid-Down (n=333)
In this section we present results specific to the opioid-down supply, therefore they may differ from the highlighted findings above that are inclusive of all expected drug categories.
- 82% of expected opioid-down samples contained fentanyl (273/333)
- 18 samples contained heroin (5% of expected opioid-down samples)
- 11 samples contained heroin (and related alkaloids like acetylmorphine (MAM) and acetylcodeine). Caffeine was found as a cut in 8 samples and erythritol (a sugar) in two samples. 7 samples were mailed-in and the other 4 were checked in Victoria.
- The other 7 samples contained heroin with the additional actives fentanyl, fluorofentanyl, bromazolam, etizolam, and lidocaine.
- 63% of expected opioid-down samples contained fluorofentanyl (209/333)
- No samples contained carfentanil
- 50% of expected opioid-down samples contained a benzodiazepine and/or etizolam (165/333)
- Xylazine was detected in 8% (27/333) of opioid-down samples
In August, 68% (266/333) of all opioid-down samples checked contained an additional active to the expected fentanyl/heroin. These data are shown in Fig. 3 highlighting the prevalence of benzos, fluorofentanyl, and xylazine in the down supply.
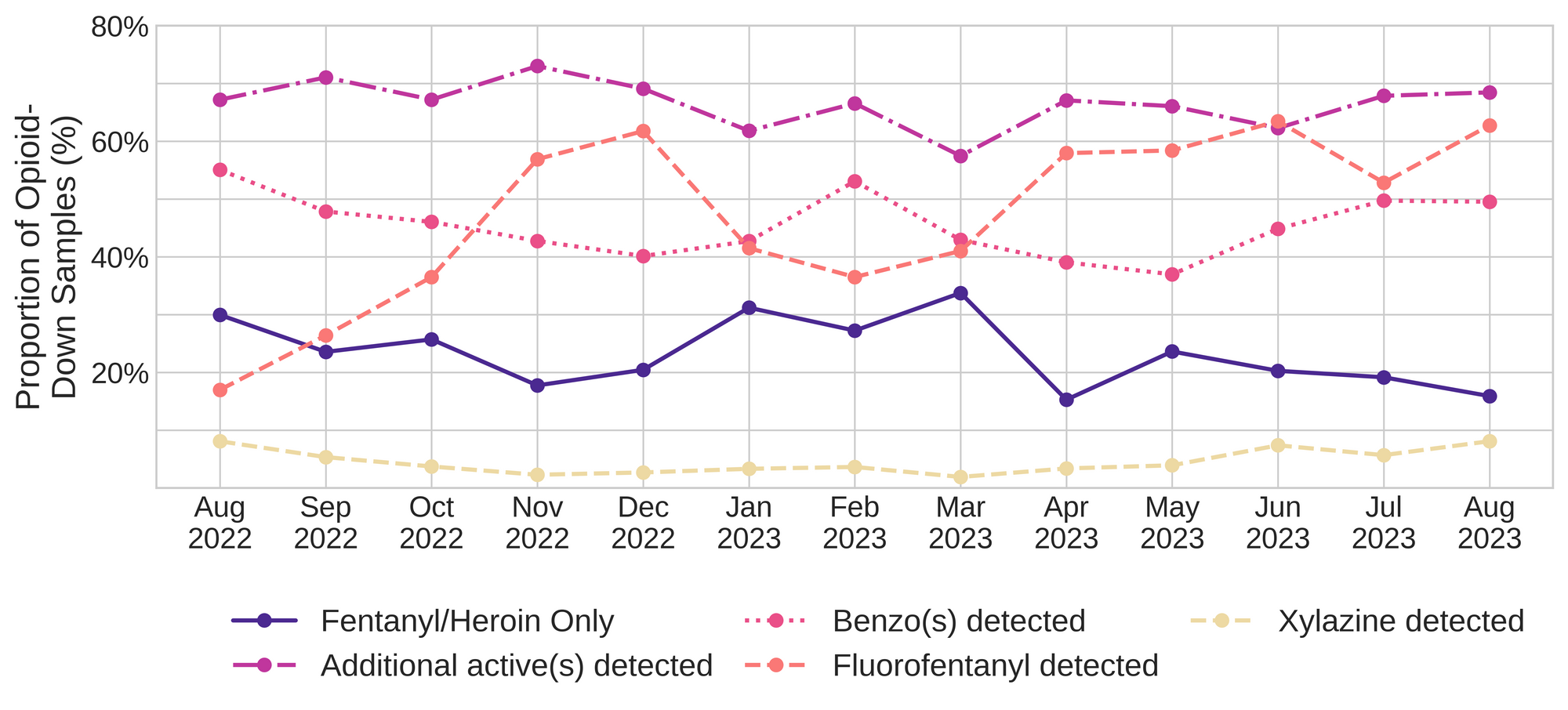
Fluorofentanyl was the most common additional active found within the opioid-down supply, with 52% (172/333) of opioid-down samples containing fluorofentanyl in addition to fentanyl. Additionally, fluorofentanyl was the only opioid detected in 21% (72/333) of opioid-down samples (i.e. no fentanyl or heroin was detected in these samples).
Benzo-related drugs contribute to a majority of the other additional actives found in expected opioid-down samples, with 50% (165/333) of expected opioid-down samples checked containing a benzo-related drug. Bromazolam continues to be the most common benzo seen in the down supply, with bromazolam being detected in 81% (134/165) of the benzo-positive opioid-down samples. Scattered detections of other drugs are still found and can be reviewed in the pdf report at the end of this blog.
Quantification for Expected Opioid-Down[1]
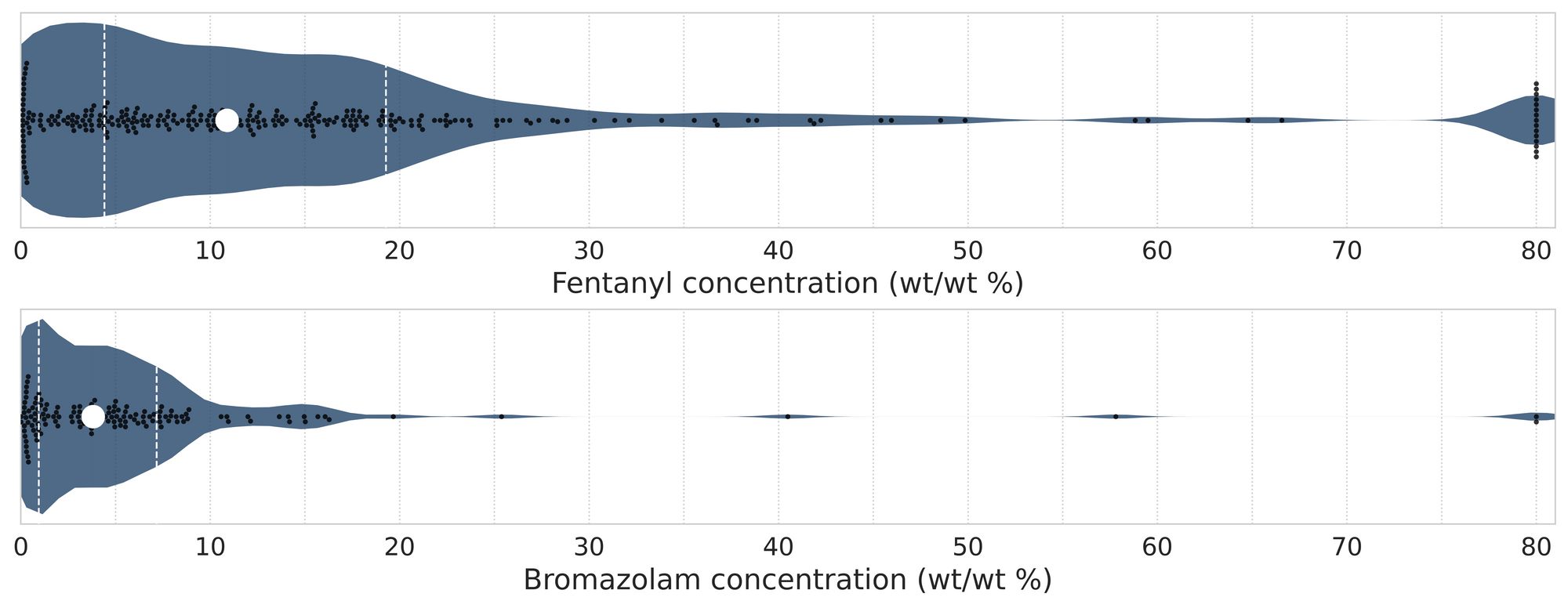
In August, we quantified fentanyl for 269 of the expected opioid-down samples containing fentanyl and found the median concentration to be 11.0%[2]. Though the median is a useful indicator, it doesn’t capture the volatility of fentanyl concentrations present in the opioid supply, as half of fentanyl-positive down samples contained between 4.4% and 19.5% fentanyl, and any one sample might be the lowest strength (0.1%) or the strongest (>80%[3]). Fluorofentanyl was seen at concentrations ranging from 0.2% to greater than 80% as well, with a median concentration of 5.1%. Similarly, the concentration of bromazolam was across the board in expected opioid down samples, with samples ranging from less than 0.1% to 57.8% bromazolam, with a median of 3.9%. For context, a sample containing 4% bromazolam would be roughly equivalent to two full 2mg Xanax bars worth of benzo per point (100mg).
Not all opioid down samples brought to our service can be quantified. This is primarily due to too limited sample collected for our instruments to report a reliable mass percentage. Nevertheless, qualitative detection is still possible. ↩︎
This number is specific to fentanyl quantified in opioid-down samples. The median concentration listed in the Key Findings at the beginning of this blog (also 9.1%) is inclusive of all samples checked, across all drug classes and unknown samples, that contained fentanyl. ↩︎
For samples that contain more than 80% fentanyl, or more than 25% etizolam by weight, our mass spectrometer is presently unable to reproducibly assign a concentration due to the upper limits of the calibration methods currently adopted. ↩︎

The fentanyl and bromazolam concentrations that we quantified in August, across all expected drug categories and service models, are presented in Fig. 4. Small black dots are individual opioid-down samples, the large white dot shows the median concentration, dashed white lines bound half of the quantified samples, and the width of the shaded regions mirrors the number of samples at a given concentration.
We can also examine the regional variability in the unregulated market. The table below expands on the quantitative data presented above. It focuses only on fentanyl, fluorofentanyl, carfentanil, bromazolam, and xylazine quantified within expected opioid-down samples, separated by collection location/model. Weight percentage is reported; “IQR” is the interquartile range: the range that contains half of the quantified samples.

Want to be notified when we release these reports? Join our mailing list to receive updates about when our reports are out. You can subscribe and unsubscribe yourself from this list at any time.
As always, send us feedback at substance@uvic.ca on how we can continue to offer our drug checking results in a useful way.